
Understanding Changes to the Vulva and Vagina: Rethinking “Normal”
Bodies naturally change over time. Physical comfort, emotional needs, body image, requirements for sexual desire, arousal, and pleasure can all be influenced by ageing. A lack of information, support, cultural myths, silencing, and negative messages can perpetuate and amplify feelings of brokenness, dysfunction, or abnormality. However, these changes are common, and variability in the experience of sexuality is both normal and healthy. They are not a loss of femininity or necessarily a sign of lack of interest in a partner.
This blog will explore the biological changes of the vulva and vagina, debunk pervasive myths, discuss the emotional and relational impact of these changes and highlight practical steps, and the importance of sex therapy.
Understanding Vulva and Vagina Changes Over Time
Step 1. If you are already scratching your head as to what I mean by “vulva” please, please, please learn this term. I’ll soon write a more detailed blog on this. The vulva is often incorrectly referred to as the vagina.
Definitions:
The vulva is the external genitalia encompassing all the external structures including the mons pubis, labia majora (outer lips), labia minora (inner lips), clitoris (another important term and area!), vestibule (vestibule contains the openings of the urethra and vagina, as well as the ducts of several glands), urethral opening, vaginal opening, and the perineum.
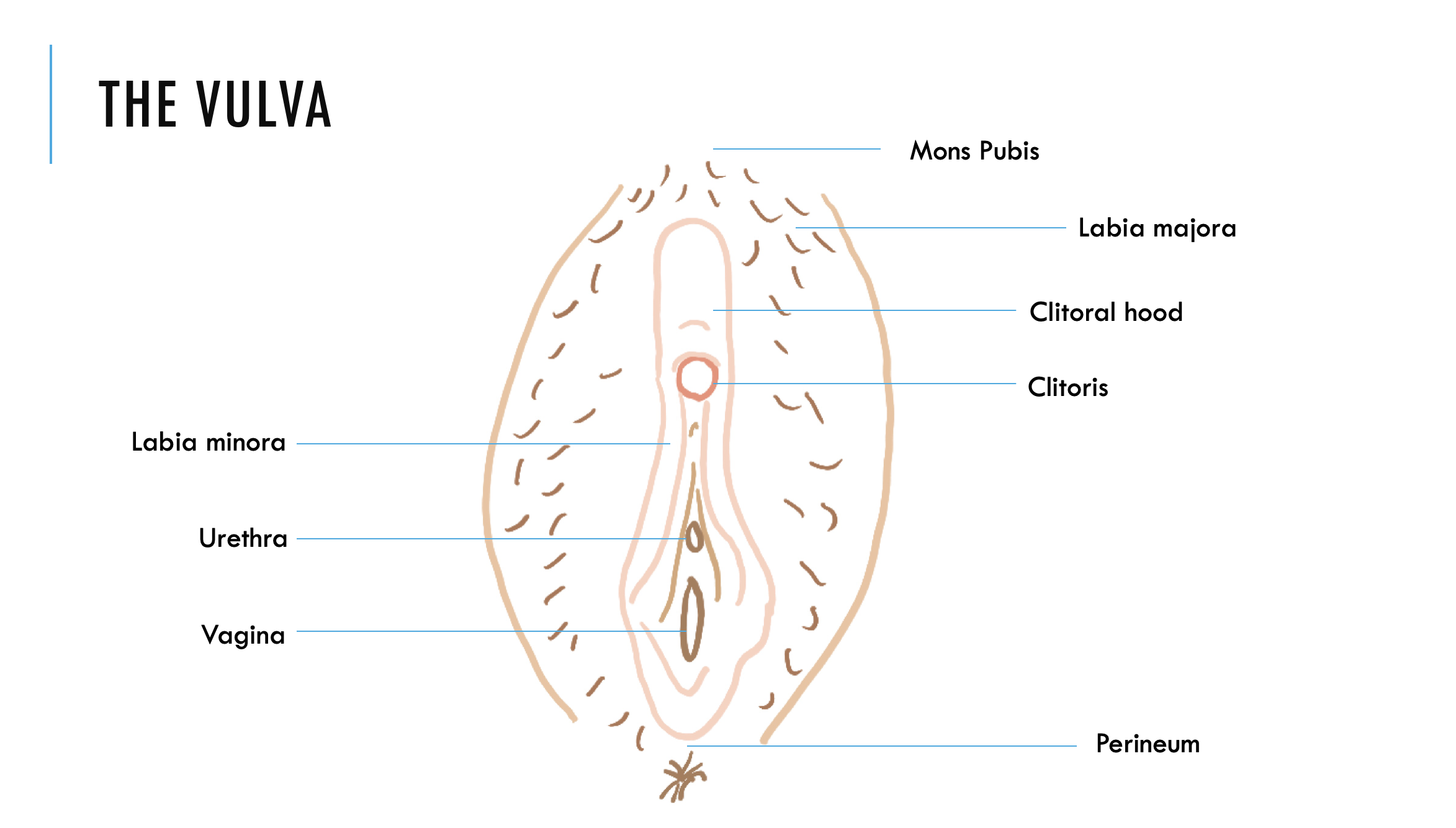
The Vulva
The vagina is the internal genital structure, which is a stretchable muscular canal extending approximately 7-13 cm up to the cervix.
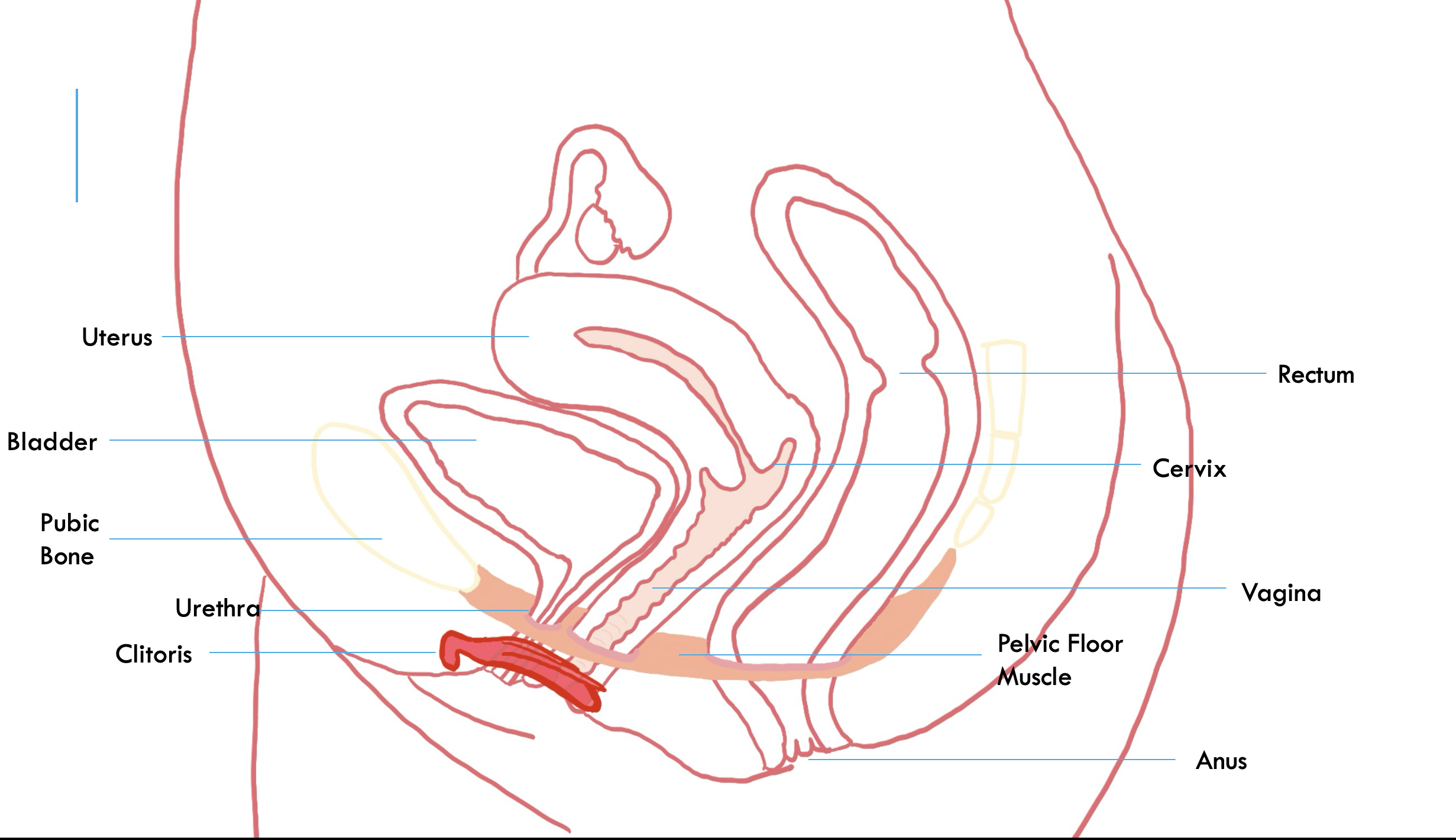
The Vagina and Internal Structures
The pelvic floor is a system of muscles that have the primary job to support vital organs in the pelvis. This includes the bladder, rectum, uterus, and vagina. It is often visualised as a hammock or bowl that holds the vital organs in place and resists downward pressure.
The clitoris is a highly sensitive structure (also worth an entire blog post or a book) which is purely for the purpose of sexual pleasure. The clitoris consists of the external glans and shaft, but the majority of the clitoris is internal and extends all the way to the vaginal opening.
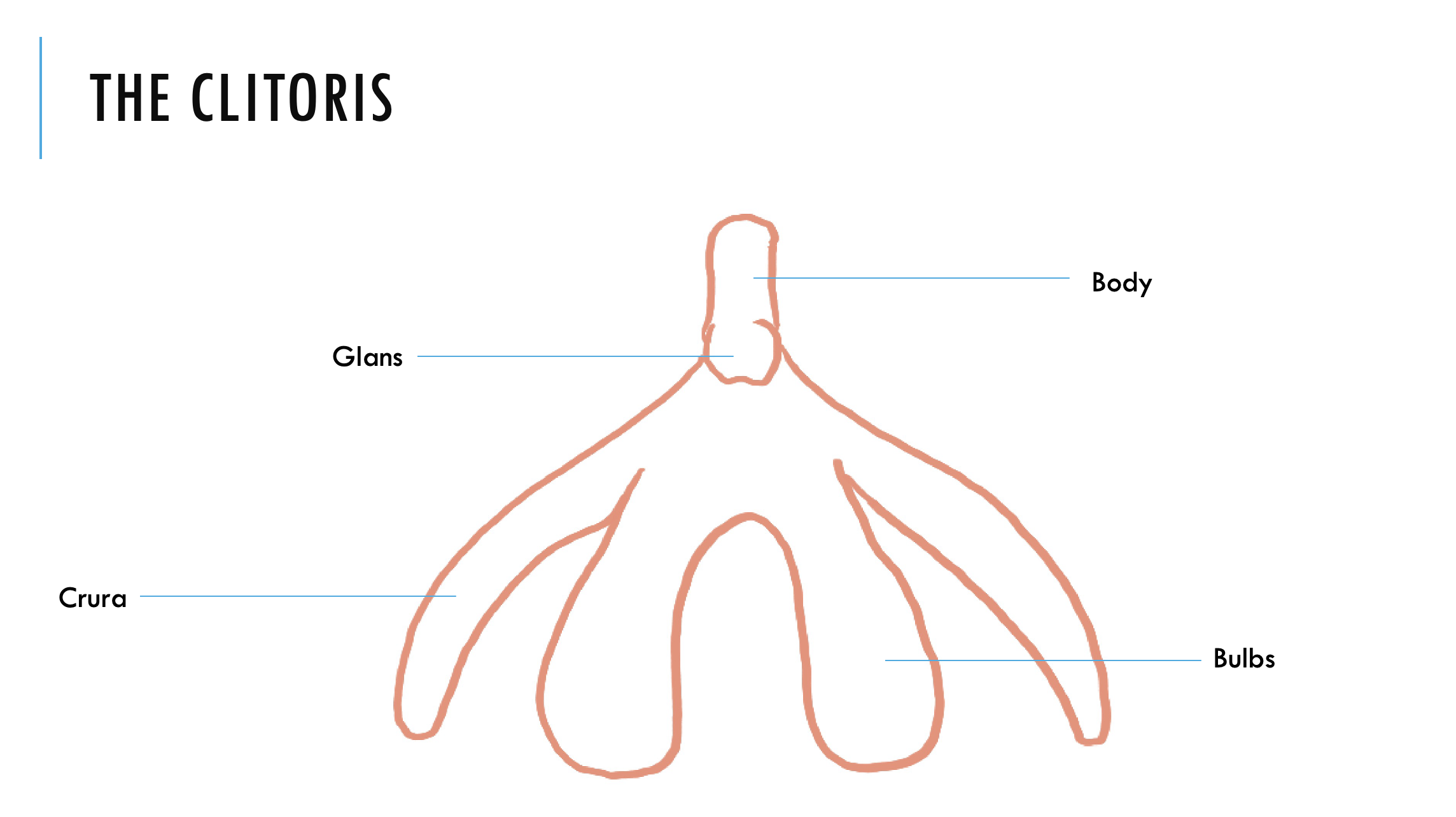
The Clitoris
Vaginal lubrication occurs during increased blood flow to the vagina during arousal. Vaginal lubrication “sweats” through the vaginal walls, and is a clear watery fluid that comes directly from the rich blood supply in the vaginal walls. Smaller amounts of mucus and thicker fluid are added to this from the Bartholin’s and Skene’s glands near the opening of the vagina. The purpose of this is to reduce friction and promote comfort during penetration.
Changes across the lifespan:
During puberty the vaginal walls thicken, the uterus grows and becomes more muscular, the vaginal pH becomes acidic as hormones shift, and the mons pubis and labia majora develop hair.
In childbirth the engorgement of the labia minora may lead to permanent enlargement. Vaginal deliveries carry the risk of pelvic floor weakness and future pelvic organ prolapse.
During perimenopause/menopause the cessation of menstruation occurs (approximately age 51) due to the dramatic decline in estrogen and progesterone. Long-term deficiencies in estrogen can contribute to chronic conditions such as Genitourinary Syndrome of Menopause (GSM).
Hormonal shifts in estrogen result in decreased blood flow to the vulva. This impacts vaginal lubrication, which reduces in quantity and speed. Postmenopausal women require longer to achieve adequate lubrication, something that can happen in 10-30 seconds for younger women. The vaginal lining thins, loses elasticity, and may atrophy. The vaginal canal becomes shorter, narrower, and the uterus and cervix shrink in size. Clitoral sensitivity can decrease progressively with age, and overall sexual response intensity decreases. There is also a decline in testosterone, the hormone largely responsible for spontaneous desire.
Slower, different arousal responses are part of natural ageing and not dysfunction. At the same time it is important to acknowledge that for some women this may bring about feelings of loss or grief, as significant changes can often bring about. Alongside this however, additional shame or feelings off brokenness often stemming from impossible standards is an unnecessary load to carry on top of these changes.
For many older adults who continue to enjoy sexual intimacy, they learn to relish in and enjoy the slower, unhurried pace of pleasure and connection. Slowing things down, can mean deeper intimacy.
When Normal Becomes Painful or Problematic
The following requires further exploration and treatment:
Painful intercourse is known as Dyspareunia. Read more about this condition here.
If pain or discomfort persists during vaginal entry or intercourse, it may indicate an underlying issue.
Genitourinary Syndrome of Menopause includes persistent symptoms of vaginal dryness, burning, itching, soreness or irritation of the vulva or vagina. Recurrent urinary tract infections (UTIs) can also be a sign of GSM due to thinning of the urethral lining.
Urinary incontinency may occur due to changes in the urethra lining and weakening pelvic muscles.
Myths About Women’s Sexual Function and Ageing
If I experience a lack of desire there must be something wrong with me: Read my blog post on low desire here. This myth is often perpetuated by the emphasis on spontaneous desire- random desire that just seems to appear. While spontaneous desire is something that does occur, responsive desire which is equally as valid and important is something that many people do not know about. Responsive desire is sensitive to contextual and relational cues, and often emerges after initiating physical contact or stimulation.
Lack of lubrication means lack of arousal or interest: This is the female equivalent of the male, “if I am turned on, I should just be able to get it up”. Vaginal lubrication is not a reliable measure of arousal. A woman can be highly aroused but lubricate slowly or minimally, or experience lubrication at times which they do not feel psychologically aroused.
Using lubricant is not natural and means something is wrong with my body: The vagina’s ability to produce sufficient lubrication changes over time. Lubricants are an effective way to enhance comfort and pleasure. Even prior to menopause, lubrication can vary and is not always reflective of arousal. No matter at what stage or age, having lubrication at hand can facilitate smoother sexual intimacy.
Ageing women lose sexual capacity and interest: Read my blog on sexuality and ageing here. While there are changes, women can still retain capacity for sexual response and orgasm long after menopause. Some older people report that sex in older age and with a long-term partner, is more satisfying than sex in youth.
Orgasm should come from penetration alone: 75% of women do not experience orgasm solely from intercourse, requiring external clitoral stimulation. I can not wait to write the blog post on this one.
The Emotional and Relational Impact
Shame, disconnection, or anxiety around changes carries a heavy toll. Many women internalise sexual difficulties as personal failures, especially if surrounded by negative sexual messages. Negative self-talk and pressure to meet impossible standards create significant stress. This in turn inhibits sexual arousal and pleasure. Many women can also struggle with negative body image, and these changes can exacerbate this. During sex, women can be distracted from intimacy by “watching” their body and its perceived flaws or performance failures. Anxiety stemming from standards of how women “should” feel can then create avoidance, which only exacerbates sexual disorders, especially pain. Without clear communication, understanding, and support, these changes can lead to unnecessary conflicts which only reinforce a woman’s negative sense of self, a lack of desire, and ultimately disconnection.
Practical Steps You Can Try Now
1. Lubricate: Incorporate lubricant (lube) into foreplay. It doesn’t have to feel disjointed, disconnected, and unsexy. Lube can be spread with fingers, exploring different strokes, pressure, and sensation. Water-based lubricant is a safe option, especially if never having used lube before. Lube may be needed more than once during sexual intimacy. Lube enhances comfort and pleasure.
2. Self-kindness: Recognise that feeling good in your body is directly linked to increased sexual wellbeing. Self-criticism which increases stress, reduces desire and arousal.
3. Regular sexual activity: This maintains blood flow to the vulva and vagina, which strengthens tissue, prevents thinning of vaginal walls, increases vaginal resilience, and exercises the pelvic floor. Sexual activity can be both partnered or solo, however, the principal of “use it or lose it” applies here.
4. Strengthen your pelvic floor: Kegel exercises in which you tense and relax the pelvic floor brings blood flow to the vaginal tissues. This supports lubrication and prevents the thinning of the vaginal walls. Healthy pelvic floor muscles also reduces urinary incontinence.
How to do a Kegel? First you need to locate your pelvic floor muscles. This can be done whilst you are urinating. As you are urinating, squeeze with the aim of stopping your urination. This might feel like a lifting up and squeezing sensation. If you slow or stop your urination by this squeeze- you have found your pelvic floor muscles (PFM). It is important to note that this should only be done to locate your PFM, and should not be done normally or regularly during urination. Now that you know where your PFM are, you can regularly practice tensing (on an inhale) and then relaxing them completely (on an exhale helps). It is important to equally focus on relaxation of the PFM, as strength and flexibility are key. Only focusing on tensing can result in tense and rigid PFM.
5. Prioritise pleasure over goal-oriented sex: Sexual intimacy is not all about sexual intercourse. Sexual intimacy can happen even without sexual intercourse. When sexual intercourse is not present, this does not mean that sexual intimacy has failed. Pleasuring, sensuality, emotional connection, erotic flow are all important components of sexual intimacy. When sexual intercourse is present: slower, longer, circular thrusting during penetration may be more enjoyable in older ager.
When to Seek Support
- If you are experiencing persistent pain (read blog here)
- If you have symptoms of vaginal bleeding, persistent burning, itching, odour, abnormal discharge, or recurring UTIs
- If pain is debilitating
- If difficulties are contributing to anxiety, depression, sexual avoidance, shame, and sexual dysfunction.
When physical symptoms are present, the first step is to seek guidance from your GP.
How Sex Therapy Can Help
Sex therapy provides a safe, non-judgemental space to explore the emotional, psychological, and relational factors that often accompany physical changes to the vulva and vagina. While medical care addresses the physical aspects, therapy supports the whole person, helping women understand and adapt to these changes with compassion rather than shame.
In therapy, we explore how beliefs, body image, and cultural messages may be shaping your experience of desire, arousal, and pleasure. We work to reduce anxiety, rebuild trust in your body, and support open communication with your partner about comfort, needs, and boundaries.
Sex therapy also encourages a shift away from performance or expectation-driven sex toward pleasure-focused, flexible, and emotionally connected intimacy. For couples, it can foster empathy, teamwork, and curiosity, replacing silence and pressure with understanding and collaboration.
For many women, this process leads to renewed confidence, body acceptance, and a richer, more authentic sense of sexual wellbeing. Therapy is about rediscovering comfort, confidence, and connection in your body as it changes. With a holistic perspective in mind, Pelvic Floor Physiotherapy may also be an integral part to treating sexual pain and experiencing renewed sexual pleasure and wellbeing.
Final Reflection/ Call to Action
Change is an inevitable and natural part of every woman’s body. These changes do not diminish your worth, femininity, or capacity for pleasure. They are invitations for new ways of connecting with yourself and those you love.
If you’re experiencing discomfort, shame, or disconnection, please know that you are not alone. Support is available. With the right combination of medical, physical, and therapeutic care, healing and renewed intimacy are entirely possible.
I offer online sex therapy across Australia, providing a confidential and compassionate space to help you understand your body, release shame, and reconnect with pleasure and confidence at any age.
Written by Justine
References:
Gambescia N, Weeks GR, Hertlein KM. A Clinician’s Guide to Systemic Sex Therapy. 3rd ed. New York: Routledge; 2021.
Torkelson C, Marienau C. Beyond Menopause: New Pathways to Holistic Health. Boca Raton (FL): CRC Press; 2023.
Quicke DLJ. Female Arousal and Orgasm: Anatomy, Physiology, Behaviour and Evolution. Singapore: Bentham Science Publishers Pte. Ltd.; 2023.
Price J. Naked at Our Age: Talking Out Loud About Senior Sex. Berkeley (CA): Seal Press; 2011.
Crooks R, Baur K, Widman L. Our Sexuality. Enhanced 14th ed. Cengage Learning; 2025.